Have you been told that the cause of your pain in your lower back is caused by a disc prolapse, based on an MRI report? Not necessarily.
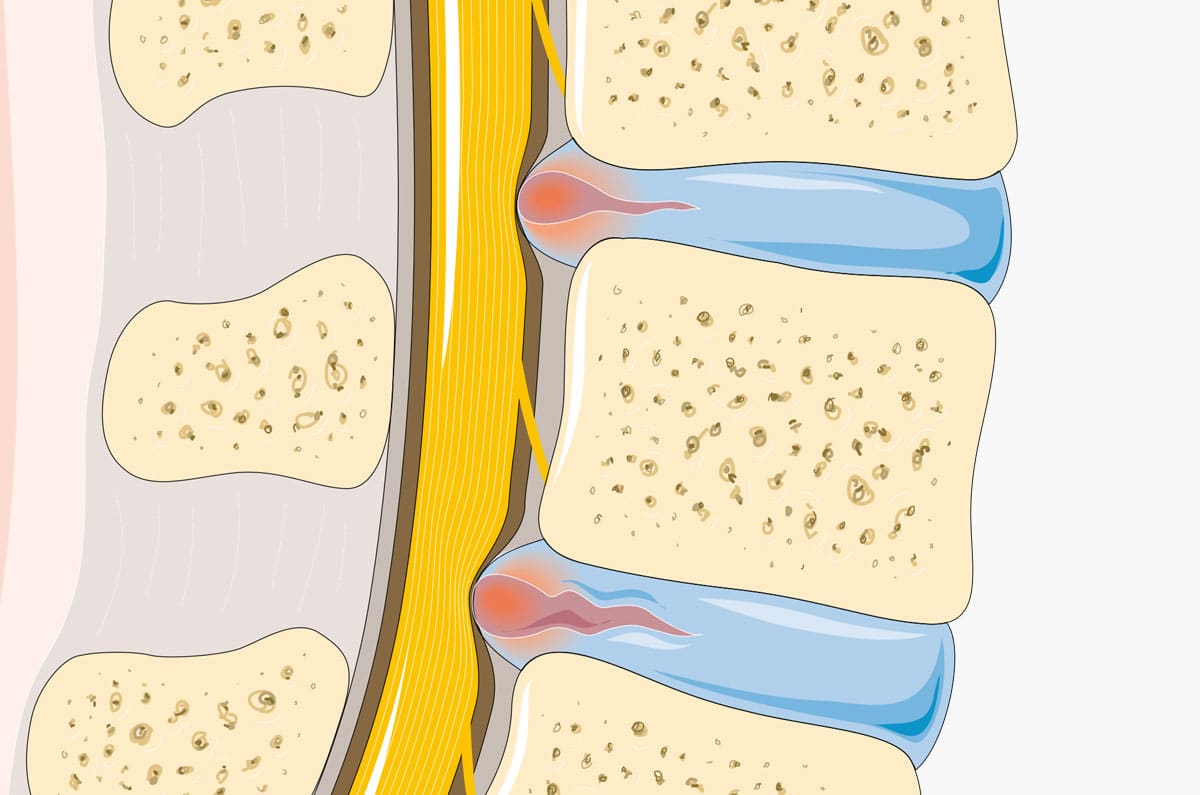
Disc prolapses become increasingly common with age. And so does low back and neck pain. Disc prolapses can press on nerve roots and cause pain to refer down the leg, at least as far down as the knee, or from the neck down the arm to the hand. Simple disc degeneration, without any pressure on the nerve root, tend to cause localised back or neck pain if any pain at all. Disc pressure on the nerve root can lead to swelling developing around the nerve root and pain radiating down the area of the limb that is supplied by that sensory nerve. Nerve root oedema can respond nicely to epidural injections, especially if the pain is of relatively new onset (lasting less than 3 months) and in younger patients. If the disc prolapse is wide enough to cause new-onset motor weakness, and especially if there is loss of urinary or bowel continence, then there is an urgent indication for surgery.
However spinal pain that radiates down the limb and the presence of a disc prolapse as seen on MRI don’t necessarily match. Thus for example, 40% of adults who undergo any spinal imaging have disc lesions, and 100% of those who reach the age of 70, even though most of these people have no symptoms of any back pain. On th eother hand, there are several biomechanical causes of spinal pain that radiate down the arm or leg and these are not seen under any imaging. Causes of pain radiating to the limb include the following (many of which are ignored):
- Pressure on a nerve root by a disc or facet joint
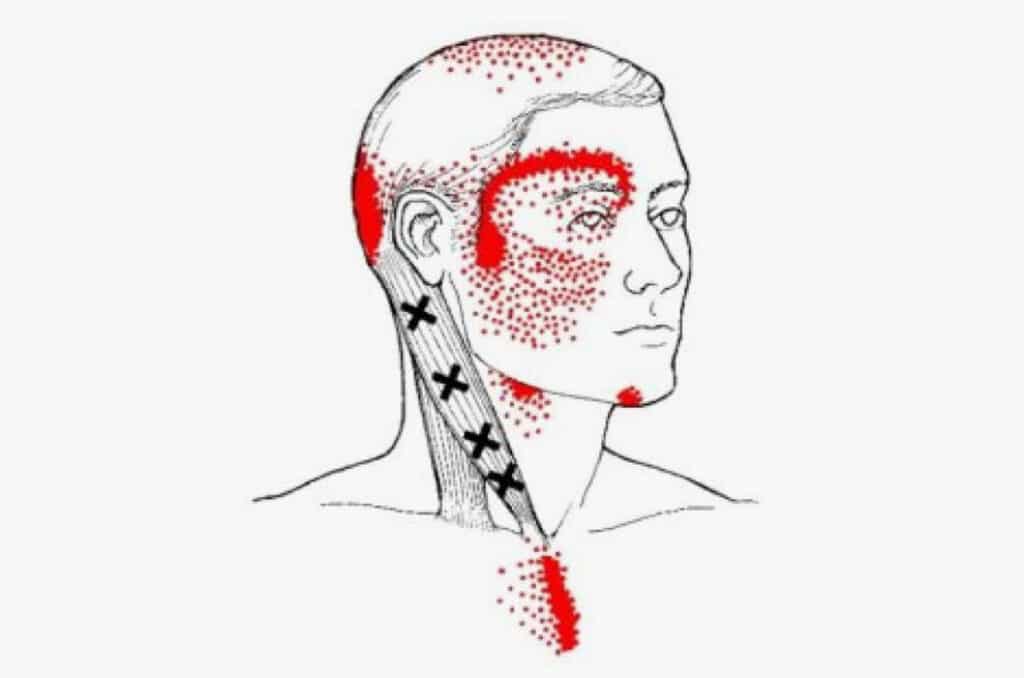
- Trigger points in various muscles
- Ligament dysfunction (especially in the sacroiliac region)
- Pain referred from the hip and shoulder joints
- Nerve entrapment by a muscle (such as piriformis, scalenes)
One must clinically evaluate these patients very methodically, especially if one is considering operative intervention. Ignorance of these less well-known causes of radiating pain will lead to treatment failure or to what we call ‘failed back surgery syndrome’. This affects between 10-40% of patients who underwent back surgery, though there are other causes for this failure. Therefore, it is absolutely necessary to confirm that the imaging findings are consistent with the clinical findings prior to any intervention, especially operative.
Generally, research on low back surgery for the treatment of low back pain and sciatica show differing results. Generally, the percentages of successful surgical results reported by orthopaedic surgeons are much higher than those reported by therapists who are not orthopedists, a factor that testifies some sort of bias towards the orthopedists. Operative success rates range from 90% improvement to no difference between those operated on and those who received other treatments, as measured after different follow-up times ranging from 2-5 years. It is important to emphasise that the success of a 2nd or a 3rd operation drop significantly and the incidence of complications rise dramatically. Therefore, it is vital to consider five times prior to a first operation, and twenty times before undergoing a second or a third.
My rules of thumb are as follows:
- Does the pain radiate down the leg, at least as far down as the knee or down the arm to the hand?
- Before deciding on having an epidural injection, or an operation on your spine, make absolutely sure that the disc is the source of your pain. Look for someone who is methodical to do that thorough clinical evaluation
- An epidural injection will not affect back or neck pain that is unrelated to nerve root pain
- An epidural injection is likely to help you if your pain has lasted for less than 3 months, as long as it fulfils the other conditions
- Seek help from someone who can assess and treat other biomechanical problems that may cause or contribute to your pain